Voice Therapy
There is currently no cure for spasmodic dysphonia, however, several treatment options exist that target voice improvement. Traditional voice therapy alone often has poor outcomes. Some patients may make slight improvements when speech is produced in small units, such as monosyllabic utterances, but improvements are rarely seen in contextual speech. There also seems to be no carryover outside of the clinical setting. However, some trial voice therapy should be done after evaluation, even if it's only used as a diagnostic tool. Some SD patients experience an easier, more efficient voice with less effort when working with an easy breath cycle, practicing yawn-sigh relaxation methods, and hierarchical analysis. It would appear, however, that voice therapy coupled with surgery or Botulinum Toxin injections results in the best therapeutic management of spasmodic dysphonia.
At present, voice therapy is recommended for the following types of patients with spasmodic dysphonia (SD):
Patients with mild, intermittent symptoms of adductor spasmodic dysphonia (SD)
Patients with a psychogenic dysphonia, psychogenic overlay, or symptom exaggeration
Patients who request assistance with increasing benefit duration following botulinum toxin injection
Patients with abductor spasmodic dysphonia (SD) who are receiving limited benefit from botulinum toxin injections
Patients who develop significant muscle tension dysphonia while trying to compensate for muscle spasm
Voice Therapy Protocol:
Voice therapy usually lasts for 6-8 sessions over 8-10 weeks. The key element in this treatment is the reduction of excessive pressure; the maintenance of a nonspasmodic phonation gives patients a sense of control over their treatment.
Focus on reducing the effort associated with voice onset by using gliding phonation with fricatives or vowels.
The program includes replacing short shallow inspirations with slow smooth inspirations, first without phonation and then with phonation. Conscious awareness of lower thoracic breath control and the rhythm of breathing are initiated. Patients are taught to use only the amount of breath needed for a particular phrase. Emphasis is placed on coordinating the lower thoracic exhalation phase of breathing with the onset of phonation.
Phrasing of 3-6 syllables is emphasized. Voiceless phonemes are added to the voiced phonemes to develop awareness in the patient that voicing is now produced more easily than in the past. Exercises to improve resonance are added after treatment for airflow control and breathing is established.
At present, voice therapy is recommended for the following types of patients with spasmodic dysphonia (SD):
Patients with mild, intermittent symptoms of adductor spasmodic dysphonia (SD)
Patients with a psychogenic dysphonia, psychogenic overlay, or symptom exaggeration
Patients who request assistance with increasing benefit duration following botulinum toxin injection
Patients with abductor spasmodic dysphonia (SD) who are receiving limited benefit from botulinum toxin injections
Patients who develop significant muscle tension dysphonia while trying to compensate for muscle spasm
Voice Therapy Protocol:
Voice therapy usually lasts for 6-8 sessions over 8-10 weeks. The key element in this treatment is the reduction of excessive pressure; the maintenance of a nonspasmodic phonation gives patients a sense of control over their treatment.
Focus on reducing the effort associated with voice onset by using gliding phonation with fricatives or vowels.
The program includes replacing short shallow inspirations with slow smooth inspirations, first without phonation and then with phonation. Conscious awareness of lower thoracic breath control and the rhythm of breathing are initiated. Patients are taught to use only the amount of breath needed for a particular phrase. Emphasis is placed on coordinating the lower thoracic exhalation phase of breathing with the onset of phonation.
Phrasing of 3-6 syllables is emphasized. Voiceless phonemes are added to the voiced phonemes to develop awareness in the patient that voicing is now produced more easily than in the past. Exercises to improve resonance are added after treatment for airflow control and breathing is established.
Medical Treatment
Recurrent Laryngeal Nerve (RLN) Sectioning Botulinum Toxin (BTX) Injections
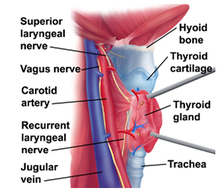
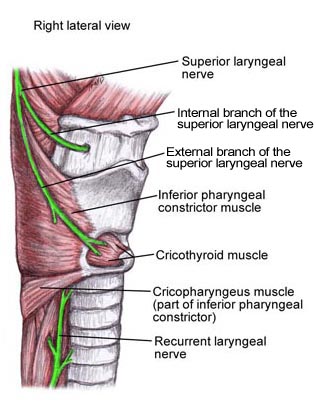
The Recurrent Laryngeal Nerve section (RLN) was the first widely used surgical procedure for spasmodic dysphonia. The recurrent laryngeal nerve is a branch of the vagus nerve that innervates the muscles of the larynx, except the cricothyroid. SD patients may be chosen for RLN section after a thorough diagnostic assessment by a surgeon and a speech-language pathologist. The patient's airflow, phonation, and voice quality are evaluated using an injection of Xylocaine. The injection is made in the RLN and produces temporary unilateral adductor paralysis. If there is a noticeable improvement in airflow and ease and quality of phonation, the decision may be made to permanently sever the RLN. After a complete recurrent laryngeal nerve sectioning, the SD patient will usually have an easily produced but breathy voice. At this point, voice therapy should focus on elevating pitch, ear training, head positioning, and digital manipulation to produce a more pleasant-sounding and efficacious voice.
|

Repeat injections of small amounts of botulinum toxin, BTX or Botox, are, at this time, the primary treatment for voice problems caused by SD. It is injected into one or both vocal folds, weakening the laryngeal muscles and resulting in smoother, less effortful voice due to less forceful closure of the vocal folds. Research by Inagi et al. has shown that the best and longest lasting postinjection voice was the result of unilateral injection toward the posterior end of the thyroarytenoid with some absorption occuring in the lateral cricoarytenoid. Breathiness and difficulty swallowing may temporarily occur for a short time after the injection. Botox injections should be followed up by voice therapy. SD patients who do receive voice therapy following injections typically retain good, functional voice for between 3-4 months, after which the symptoms usually return. Reinjections are necessary to maintain good speaking voice. Initial side effects of the injections include a temporary weak, breathy voice or occasional difficulties with swallowing. Voice therapy should focus on decreasing these effects and reducing vocal hyperfunction.
|
Contraindications
Contraindications and relative contraindications to botulinum toxin therapy are as follows:
- Pregnancy: Use of botulinum toxin by women who are pregnant or lactating is not recommended.
- Aminoglycosides: Recent use of aminoglycosides interferes with neuromuscular transmission and may increase the effect of the botulinum toxin therapy. The authors recommend that patients receiving aminoglycoside treatment not receive concurrent botulinum toxin injections.
- Gastroesophageal reflux: Administer antireflux therapy in patients with known or suspected reflux before considering botulinum toxin injections. Botulinum toxin injections reduce the speed of vocal fold closure and may predispose the patient to aspiration.
- Preexisting neurologic disorders (eg, myasthenia gravis, Eaton-Lambert syndrome, motor neuron disease affecting the neuromuscular junction): Use caution when administering botulinum toxin to patients with these disorders, especially when large doses are required. Although the amount of toxin that enters the systemic circulation after injection is minute, hyperkinetic symptoms could theoretically occur.
Future and Controversies
Surgical therapy for spasmodic dysphonia (SD) is still controversial because the side effects can be severe, and wide evaluation with long-term follow-up data is not available.
To date, botulinum toxin injection is the standard therapy for spasmodic dysphonia (SD). Unfortunately, this is just a treatment at the end organ and is not a cure. The key to understanding this disorder is to understand its pathophysiology and that of other spasmodic movement disorders.
Current research, especially gene research, is progressing in the elucidation of the cause of focal dystonia. Advances in the understanding of genetically determined early-onset primary torsion dystonia are offering insight into the pathophysiology of dystonia. An amino acid deletion in the DYT1 gene has been found to be responsible for familial primary torsion dystonia. This defect results in an abnormality in the protein torsinA, which is widely distributed in the CNS. Further investigation of the of this gene and its protein products will hopefully spur advances in our understanding of dystonia and improve our treatment of the disorder.
To date, botulinum toxin injection is the standard therapy for spasmodic dysphonia (SD). Unfortunately, this is just a treatment at the end organ and is not a cure. The key to understanding this disorder is to understand its pathophysiology and that of other spasmodic movement disorders.
Current research, especially gene research, is progressing in the elucidation of the cause of focal dystonia. Advances in the understanding of genetically determined early-onset primary torsion dystonia are offering insight into the pathophysiology of dystonia. An amino acid deletion in the DYT1 gene has been found to be responsible for familial primary torsion dystonia. This defect results in an abnormality in the protein torsinA, which is widely distributed in the CNS. Further investigation of the of this gene and its protein products will hopefully spur advances in our understanding of dystonia and improve our treatment of the disorder.
Sources:
Boone, D.R., McFarlane, S.C., Von Berg, S.L., & Zriack, R.I. (2010). Neurogenic voice disorders. The Voice and Voice Therapy (98-104). Boston, MA: Allyn and Bacon.
Inagi, K., Ford, C.N., Bless, D.M., & Heisey, D. (1996). Analysis of factors affecting botulium toxin results in spasmodic dysphonia. Journal of Voice, 10, 309-313.
Murray, T., & Woodson, G.E. (1995). Combined-modality treatment of adductor spasmodic dysphonia with botulinum toxin and voice therapy. Journal of Voice, 9, 460-465.
Pitman, M., Kamat, A., Bliznikas, D., & Baredes, S. (2013). Spasmodic dysphonia. Retrieved from http://emedicine.medscape.com/article/864079- overview
Boone, D.R., McFarlane, S.C., Von Berg, S.L., & Zriack, R.I. (2010). Neurogenic voice disorders. The Voice and Voice Therapy (98-104). Boston, MA: Allyn and Bacon.
Inagi, K., Ford, C.N., Bless, D.M., & Heisey, D. (1996). Analysis of factors affecting botulium toxin results in spasmodic dysphonia. Journal of Voice, 10, 309-313.
Murray, T., & Woodson, G.E. (1995). Combined-modality treatment of adductor spasmodic dysphonia with botulinum toxin and voice therapy. Journal of Voice, 9, 460-465.
Pitman, M., Kamat, A., Bliznikas, D., & Baredes, S. (2013). Spasmodic dysphonia. Retrieved from http://emedicine.medscape.com/article/864079- overview
